

A Dietary Guide to Cancer Defense
From menus and meal plans to cellular microenvironments

While cancer encompasses a wide spectrum of diseases, certain hallmarks are common among them, such as resistance to cell death, sustained proliferative signaling, and reprogramming of energy metabolism. One critical trait is acquired resistance to apoptosis.
Cancer at the Cellular Level: Apoptosis vs. Necrosis
Under normal conditions, cells that fail to pass certain checkpoints during the cell cycle are marked for programmed cell death via apoptosis, a form of cellular suicide that removes damaged or unwanted cells without causing inflammation.
Cells that die in this manner slowly shrink and leave surrounding tissue intact—“not with a bang but a whimper.” Apoptosis serves as a natural barrier to cancer development, and its suppression can promote tumor growth.
In contrast, necrosis involves the rupture of the cell membrane, leading to the release of proinflammatory cytokines into the surrounding tissue microenvironment, akin to a supernova explosion.
This process triggers inflammation and recruits immune cells to the site of damage, which stimulates angiogenesis, the formation of new blood vessels that supply oxygen and nutrients to tumors and facilitate their growth.
The tumor microenvironment consists of surrounding noncancerous cells and molecules, which are often cajoled by cancer into acting as accomplices. If a given microenvironment was characterized by apoptosis as the dominant form of cell death over necrosis, that microenvironment could preclude the development of cancer.
Key Questions
If cancer development is driven by the tumor microenvironment, how can an individual’s broader macroenvironment impact cellular microenvironments?
Can dietary choices help maintain appropriate levels of apoptosis and thus reduce cancer risk?
Cancer Is Not Caused by Mutations

“We find ourselves at the present time in the era of molecular biology, and we are perhaps unduly influenced by the genetic code as the dominant principle in biology. Perhaps, in a decade or two from now, the dominant principle may shift to another plane, which in turn will influence our speculations about tumor causation.”
The Impact of Cruciferous Vegetables on Cancer Risk
Cruciferous vegetables—such as broccoli, cabbage, kale, and Brussels sprouts—are rich in compounds that have been shown to induce apoptosis in various in breast, brain, blood, bone, colon, gastric, liver, lung, oral, ovarian, pancreatic, prostate, and skin cancer lines.
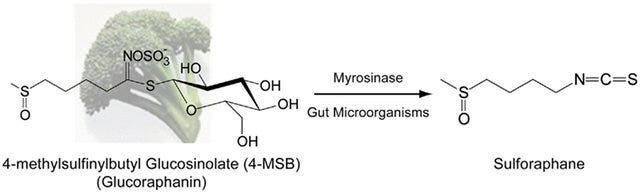
One such compound called sulforaphane, particularly abundant in broccoli sprouts, bok choy, and cabbage, also induces apoptosis in acute lymphoblastic leukemia (ALL), the most common blood cancer in children.
Optimizing Sulforaphane Intake
A 2008 randomized controlled trial found that consumption of raw broccoli resulted in faster absorption, higher bioavailability, and higher peak plasma amounts of sulforaphane compared to cooked broccoli.
Boiling, steaming, or microwaving at high power (850–900 watts) can inactivate myrosinase—a plant enzyme essential for converting glucosinolates (like glucoraphanin) into biologically active isothiocyanates (like sulforaphane).
To enhance sulforaphane bioavailability when consuming cooked vegetables, one can:
Add powdered brown mustard seeds, a rich source of myrosinase, to cooked broccoli
Rely on colonic gut microbiota, which possess myrosinase enzymes, to facilitate the conversion of glucoraphanin to sulforaphane, albeit to a lesser extent than would occur in the small intestine
Recent studies continue to support the potential anticancer effects of sulforaphane. For example, a 2023 Frontiers in Oncology review highlighted sulforaphane's antioxidant, anti-inflammatory, cardioprotective, immunostimulant, and anti-cancer properties. However, most clinical studies are limited and focus on biomarkers rather than long-term cancer outcomes. More extensive human clinical trials are needed to fully understand the impact of sulforaphane on cancer prevention.
Resistant Starch & Colorectal Cancer Prevention
Colon cancer is the third most common type of cancer globally and remains a leading cause of cancer-related deaths. Particularly concerning is the recent rise of colon cancer among young adults. Dietary patterns significantly influence colorectal cancer risk, with fiber intake being inversely associated with disease incidence. In fact, immigrants experience an increased risk of colon cancer after moving to developed countries and converting to a Western diet.
Resistant starch (RS) refers to starch that escapes digestion in the small intestine and reaches the colon undigested, where it is fermented by gut microbiota to produce short-chain fatty acids (SCFAs) like butyrate. Butyrate serves as the primary energy source for colonic epithelial cells and has anti-inflammatory and anticancer properties. The short-chain fatty acid promotes apoptosis in mutated cells, inhibits cell proliferation, and improves gut barrier function.

Not All Fiber Is Created Equal
In contrast to other types of fiber such as non-starch polysaccharides (NSP), resistant starch may confer unique benefits and can be characterized into five types, the first three of which occur in a normal human diet:
RS1 describes starch that is physically trapped within plant cell walls and protein matrices and includes whole grains, seeds, and legumes
RS2 consists of native, granular starch and includes green bananas, raw potatoes, and high amylose corn starch
RS3 comprises retrograded starches that are formed when starchy foods (e.g. rice, potatoes, pasta, bread, cornflakes) are cooked and cooled
RS4 is composed of chemically modified starches used in the food industry to commercially produce baked goods
RS5 refers to amylose-lipid complexes, consisting of starch and fatty acids, that form during food processing, which may include the use of emulsifiers
RS2, such as raw potato starch, ferments quickly in the proximal part of the colon, and doesn’t change stool pH. On the other hand, RS3 ferments slowly all the way to the distal end of the colon and feeds SCFA-producing bacteria, thereby lowering colonic pH, preventing pathogen invasion, maintaining epithelial tissue health, and inhibiting carcinogenesis. Most of the fiber content in a typical Western diet primarily ferments in the proximal portion of the colon.
Studies have shown that individuals with colorectal cancer often possess lower levels of butyrate-producing bacteria, such as Faecalibacterium prausnitzii and Roseburia species, compared to healthy individuals. A study examining the effects of resistant starch using human gut microbiota cultures found that RS3 doubled the proportion of Bifidobacterium in the distal colon and induced higher levels of butyrate production.
The most common example of RS3 is cooked and cooled rice and potatoes, but green plantains, cassava, and taro also contain mixtures of several types of resistant starch, including RS3. Although specific daily intake recommendations for resistant starch have not been formally established, evidence suggests that:
Approximately 20 grams of resistant starch per day may confer digestive health benefits
6 to 12 grams per meal can inhibit postprandial increases in blood glucose and insulin levels
In contrast, the average American intake is estimated to be around 4.9 grams per day, slightly below the range needed to observe beneficial effects at a single meal and considerably short of the daily intake associated with health benefits.

Red Meat Consumption & Colorectal Cancer Risk
The relationship between red meat consumption and colorectal cancer has been extensively studied, with mixed findings:
